





















Schedule One
Inside the medical cannabis movement in Iowa and across the country.

This story has been updated to reflect new laws regarding medical and recreational cannabis put into place on November 8th.
Margaret Gaer, a 26 year old from West Des Moines, began using hemp oil 19 months ago, but she’s suffered from Dravet syndrome, a severe form of epilepsy, almost all her life. Before using hemp oil, Gaer tried multiple prescription medications to treat her seizures, including two to counter the effects of the seizure medications themselves.
After Iowa legalized the use of cannabidiol (CBD) oil for intractable epilepsy in May 2014, Gaer applied for a cannabidiol card. However, because the legislation passed did not permit CBD oil to be produced in Iowa, Gaer had to reach outside of the state for treatment.
“We had to wait, even though we had her cannabidiol card under Iowa. We had to wait until we were able to get it from Colorado,” Margaret’s mother, Sally Gaer, said.
Sally Gaer is a representative for Iowans 4 Medical Cannabis, a coalition made up of patients of a number of conditions as well as caregivers, physicians, and family members. The coalition supports a comprehensive program that would broaden the currently relatively limited legal uses of medical cannabis in Iowa.
“I hope this legislative session we are able to get a comprehensive medical cannabis program in Iowa where the medical cannabis can be grown, produced, tested, and dispensed in Iowa, for Iowans, for diseases that physicians determine, not legislators,” Gaer said.
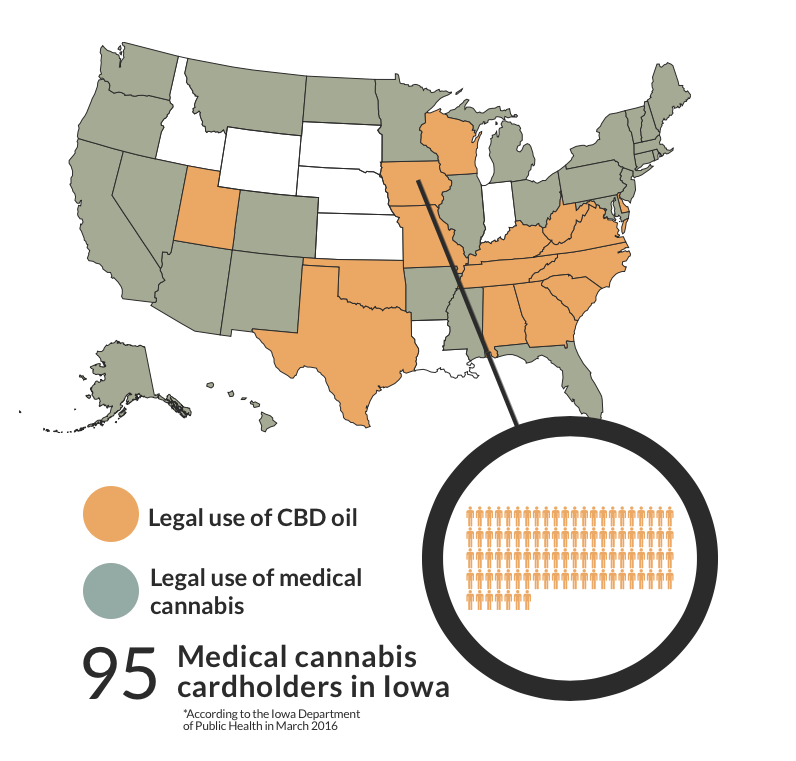
In total, 43 states allow for medical use of cannabis to some degree. Iowa is currently one of 15 states to legalize the use of CBD oil, a non-psychoactive extract of cannabis, for medical uses. CBD oil does not contain THC and therefore does not give patients a high. 28 states currently allow medical use of the actual cannabis plant.
Beyond these two categories, individual state laws can vary enormously. Iowa, for example, is the only state in which CBD oil cannot be produced, despite being legal for Intractable Epilepsy, and no legal dispensaries exist in the state. By contrast, California permits medical cannabis for any illness for which it can provide relief, and companies like Eaze can deliver it right to a patient’s doorstep.
Mae Van Der Weide ‘16 currently works as a model in Los Angeles. In recent months, Van Der Weide has been involved with nonprofit organization Grow for Vets, which donates medical cannabis to veterans in need.
“I got involved with medical marijuana because I saw its potential to help cancer and PTSD patients instead of taking a cocktail of unnecessary medication,” she said.
Having lived in both Iowa and California, Van Der Weide can attest to the difference in perception in the two states surrounding the plant.
“The attitude toward cannabis in Iowa is incomparable to that of California. California always takes the lead with progressive policies,” she said. “It’s only a matter of time before medical marijuana fully makes its way to the Midwest.”
This variance comes in part due to the federal regulations surrounding the drug. Marijuana is currently classified as schedule one, meaning it has no accepted medical uses and a high potential for abuse, according to the DEA. Other schedule one drugs include Heroin and LSD.
Carl Olsen, an application developer at Drake University and cannabis blogger, has been actively involved in numerous petitions at the national level to have marijuana rescheduled and recognized for its medical merits, including the 2002 petition filed by the Coalition for Cannabis Rescheduling. This petition eventually ended in the US Court of Appeals in 2013.
“Now it’s just more of a residual stigma. That stigma’s kind of going away, but how do you undo all of that international law and federal law?” he said. “[The DEA and federal government] put so many obstacles that it’s really hard to reverse all of that.”
Because marijuana is a schedule one drug, research at a federal level is highly restricted. However, research does exist on a smaller scale. Frank Caligiuri is a professor of pharmacy and board certified pharmacotherapy specialist. He has spoken on panels at the state capital regarding the medical uses of cannabis.
“When it comes to cannabinoid research, looking at the compounds found in cannabis such as THC and cannabidiol, the list goes on and on. You name it, there’s plenty of research. It’s just that most of that research is at a subclinical level, a level of animals,” Caligiuri said. “But in most of those studies, whether it’s looking at inflammation, pain, Crohn’s disease, or certain types of cancers, there’s certainly plenty of literature to suggest at a cellular level, this is what’s happening, and it’s the cannabinoids that are primarily doing that.”
I got involved with medical marijuana because I saw its potential to help cancer and PTSD patients instead of taking a cocktail of unnecessary medication
— Mae Van Der Weide
For as long as marijuana remains a schedule one drug, its legal use will largely be left up to the states. A bill that would have permitted Iowans to attain CBD oil in Minnesota as a means of keeping production out of Iowa while still granting patients access was shot down by the Iowa House last April. The bill would not, however, have changed the fact that transporting marijuana across states lines is a federal felony.
Caligiuri emphasizes the importance of having medical professionals at the center of medical cannabis programs. There are currently three states, Connecticut, Minnesota, and New York, where cannabis is dispensed to patients by pharmacists themselves.
“For people like myself, I think that’s the ideal situation, to have health care professionals involved in the entire process and not just going to a dispensary,” Caligiuri said.
One of the keys to a responsible medical cannabis program lies in having a patient registry, according to Caligiuri.
“States that do have a program should have a registry where all patients can sign up so we know what other drugs they’re taking and drug interactions and things like that. States that have models and have a medical board that approves or removes certain conditions based on the evidence is the ideal model to have,” he said.
Because CBD oil is only available to epilepsy patients in Iowa, part of the initiative for groups like Iowans 4 Medical Cannabis includes expanding the legal list of conditions. Aimee Loats has suffered from Crohn’s disease since the age of 10.
“When I was first diagnosed, there weren’t a lot of medical options. I started taking these heavy steroids and it altered my joints, growth and puberty. I definitely suffered a lot of other side effects,” the 22 year old student at Simpson College said. “I just remember thinking that if I could have avoided that I could have avoided a lot of long term side effects.”
Now an advocate herself for medical cannabis reform in Iowa, Loats believes part of the resistance to the movement lies in stigma surrounding the drug.
“Now that this is becoming more of a movement, it’s something that I’ve developed a passion for. I want to bring to people’s attention that this is not about the stigma of getting high or using it for recreational use,” she said. It’s about people who don’t have any other options and would benefit from cannabis more than having extreme side effects from FDA approved drugs.”
To know how cannabis actually affects the body, it’s essential to understand the endocannabinoid system, named after the plant that helped lead to its discovery. This system is made up of endocannabinoid receptors and endocannabinoids, which stimulate the receptors. They are located throughout the body in the cell membranes and work between the body’s various systems, allowing for communication between different kinds of cells.
Phytocannabinoids are plant substances that stimulate these receptors. One of the most well-known phytocannabinoids is THC, or tetrahydrocannabinol.
“If you understand or at least know there are endogenous receptors in your body where compounds like THC work on a daily basis to regulate your sleep or appetite, you may have a better appreciation for how those cannabinoids can work in medicine,” Caligiuri said.
Another bill introduced to the House Ways and Means Committee last legislative session is House File 2384. This bill would have allowed for two dispensaries in Iowa and add multiple sclerosis and terminal cancer with a life expectancy of less than a year to the list of accepted diseases. The bill was stalled in the House Ways and Means committee, then sent to the Public Safety Committee to never be addressed.
After the bill allowing Iowans access to medical cannabis produced in Minnesota failed, Governor Terry Branstad said he feared producing CBD oil in Iowa would lead to “unintended consequences.”
“People who want it recreationally are not going to pay the price that it costs in a medical dispensary,” Gaer said. “A recreational user cannot get access in a dispensary, so there’s no way the recreational use goes up.”
For an activist like Gaer, reluctance to embrace medical cannabis programs from lawmakers is a major obstacle.
“I’m very frustrated by legislators that fail to do their homework and become educated that this is a treatment option,” she said. “I’m very frustrated that they feel we need FDA trials on everything when there’s very dangerous drugs out there that have been through FDA trials and are killing people.”
The stigma carried by cannabis was a cause for question and concern for Olsen.
“I had heard so many negative things about [marijuana] that I was trying to figure out why they would lie about it. It put me in a position where I started to get extremely afraid. I just thought this is such a wild thing that they have created all this hatred toward this plant,” he said. “ I thought once you discover something that evil you can’t really go along with it, you have to protest.”
I’m very frustrated by legislators that fail to do their homework and become educated that this is a treatment option
— Sally Gaer
With eight states having currently legalized marijuana for recreational use, the attitude toward the drug is undoubtedly shifting in the US. However, Gaer maintains that recreational and medical use are separate issues and should be treated as such.
“[There is] a misconception that we’re asking for recreational use, and we are not. There are so many delivery methods, oils patches, creams,” she said. “People do not need to smoke to get the benefit. It’s the old mindset that people are sitting around smoking it when that’s not true.”
Your donation will support the student journalists of Iowa City High School. For 2023, we are trying to update our video and photo studio, purchase new cameras and attend journalism conferences.